Boosting Survival Rates
For the first time in nearly 40 years, we have the ability to reduce the number of deaths from sudden cardiac arrest in the workplace.
- By C. J. Palmer, NREMT-P
- Jun 01, 2005
 SUDDEN cardiac arrest takes more than 460,000 lives in the
United States each year. Despite prompt recognition of the event and
immediate CPR, survival rates of less than 5 percent are still
commonplace. And despite decades of training first responders and community members in cardiopulmonary resuscitation (CPR), the death rate from out-of-hospital cardiac arrest has changed very little in the past 35 years.
SUDDEN cardiac arrest takes more than 460,000 lives in the
United States each year. Despite prompt recognition of the event and
immediate CPR, survival rates of less than 5 percent are still
commonplace. And despite decades of training first responders and community members in cardiopulmonary resuscitation (CPR), the death rate from out-of-hospital cardiac arrest has changed very little in the past 35 years.
For the first time, however, we have the ability to reduce the number of deaths from sudden cardiac arrest in public venues and the workplace. Recent studies reveal approximately 80 percent of all adult sudden cardiac arrest victims will have cardiac rhythms that are potentially "shockable" in the first few minutes after their hearts stop beating. Defibrillation is the only effective method to treat these lethal cardiac rhythms.
Defibrillation is the process in which an electronic device (a defibrillator) gives a specialized electrical shock to the heart. A defibrillator clears the heart's electrical system (a reboot of sorts), allowing the heart to re-establish a normal rhythm. This is the only treatment when the heart is in cardiac arrest from the most common causes, ventricular fibrillation and ventricular tachycardia. These chaotic heart rhythms need to be stopped so the heart has a chance to resume normal electrical activity and begin pumping blood again.
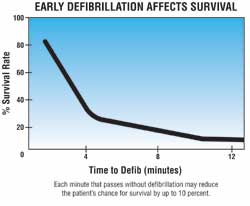
The chance of surviving cardiac arrest is decreased by 7-10 percent with each minute that passes after collapse. National studies and position statements from leading emergency
physician groups show the emergency medical services (EMS) call time to defibrillation time usually exceeds 10 minutes. This is supported by a rather dismal resuscitation rate of less than 5 percent for out-of-hospital cardiac arrest in most communities. A 1996 study in Chicago showed there was less than a 1 percent chance of surviving out-of-hospital cardiac arrest in that city, and other large metropolitan cities have reported similar statistics.
Defibrillation provides the single most important therapy for the treatment of cardiac arrest in the adult patient. Resuscitation science now places great emphasis on early and rapid delivery of both CPR and defibrillation. The chances of survival are greatly enhanced when the interval between the start of cardiac arrest and the delivery of defibrillation is as brief as possible.
Impact of EMS Response Times
Research studies show well more than half of cardiac arrest victims could be saved if they were treated rapidly with defibrillators. In some studies, the results were even more dramatic. Prompt response by EMS with rapid defibrillation capability increases survival rates to only 5 percent. While those who deliver emergency medical services frequently tout their rapid response times, it is difficult to get EMS providers at the side of the cardiac arrest victim in less than five minutes.
Response times are traditionally measured from the time of dispatch to arrival at the address. This does not take into account the time it takes to reach the patient. Studies show response times to local businesses may well be within five or 10 minutes, but the time it takes to access the patient, assess the situation, and deliver defibrillation is closer to 10-12 minutes. At this point the chances for survival, even when CPR is being performed, are significantly reduced. The national standard on which EMS providers gauge service delivery success is usually eight minutes. This is often the average response time, not a goal for every call.
On-site AEDs can be positioned in most business settings so that trained first responders can access the unit and deliver defibrillation in three to four minutes. This is what accounts for the significant number of "saves" in settings where AEDs are present. The presence of trained, on-site emergency responders who have an AED immediately available tremendously improves survivability from cardiac arrest in the workplace.
At O'Hare International Airport in Chicago, none of the 60 to 70 cardiac arrest victims they see each year survived the event, despite having paramedics stationed at the airport, in a three-year study period. The airport installed 33 AEDs, trained minimal numbers of personnel, and relied on a trained public to react in the event of cardiac arrest. The survival rate at O'Hare is now 64 percent, and 10 of every 11 survivors in the initial study were still at their pre-arrest level of function one year after their cardiac arrest.
This level of out-of-hospital success in resuscitation is not the norm in medicine. Even the most seasoned health care professionals found the O'Hare numbers hard to believe, primarily because they have never seen such success in their clinical practice setting. Yet the benefit of early defibrillation, prior to arrival of EMS, has since been demonstrated in several studies with results very similar to the O'Hare study.
From a business standpoint, AEDs return workers to the workplace. They reduce lost time and return a productive worker to the company in a relatively short period of time. This is the primary reason for the emphasis on early defibrillation by every agency involved in providing emergency response training.
Return to a Productive Lifestyle
One area frequently overlooked by companies is the long-term benefit of an AED program. While initial costs of equipment and training can be substantial, the program can be very cost effective. Much like investing in fire extinguisher to control a small fire so it does not devastate a business, the AED and trained worker can not only save a life, but the cardiac arrest victim who is defibrillated early more often than not survives to return to a productive lifestyle.
In emergency medicine, success is usually measured in the ability to convert a pulseless patient into one who has a pulse. This concept of "saving the patient" often does not evaluate the survivability for the long term or the ability of the patient to return to a normal lifestyle. While many "saves" are obtained by paramedics and emergency department staff, long-term survival and return to a normal lifestyle is very low. The opposite is true when rapid defibrillation has occurred in settings where persons are trained in CPR and an AED is present.
National and International Guidelines
While today's paramedic systems are frequently able to obtain a heartbeat on many patients, the delays in delivery of care often result in only short-term survival because of extensive damage to the heart and brain that is caused by the lack of oxygen. To achieve the earliest possible defibrillation, the International Liaison Committee on Resuscitation (ILCOR) endorses the concept that automated external defibrillators should be placed in public and workplace settings, including advocating their use by non-medical trained persons. ILCOR recommends personnel be authorized, trained, equipped, and directed to operate a defibrillator if their responsibilities require them to respond to emergency situations, including persons in cardiac arrest. This recommendation includes all first responder emergency personnel, both in the hospital and in out-of-hospital settings.
OSHA has issued a recommendation that workplace settings should provide AEDs for use in emergency situations. The American Health & Safety Institute, American Heart Association, American Red Cross, and National Safety Council all endorse and support the concept of early defibrillation in both public and workplace settings through their training programs. Advanced resuscitation training programs (ACLS and PALS) for health care professionals now mandate AED training as a vital component of the program.
While many tout the exceptional success seen with AED programs, the quality of CPR training and presence of trained first responders in industry settings should not be overlooked. On-site emergency responders are most likely to be the only ones to provide care for a victim in the first few minutes. They should be trained to respond and provide assistance prior to arrival of emergency medical services. Untreated heart attacks can progress to the point where the heart stops pumping blood.
Heart attacks are the leading adult medical emergency in the United States. Some 743,000 people died last year from coronary heart disease, making it the leading cause of death in the United States. On the positive side, survival from a first-time heart attack--without cardiac arrest--has increased dramatically. The acceptance and increased use of cardiac catheterization and "clot buster" drugs, along with increased training for EMS providers and the lay public, has significantly increased heart attack survival rates. While resuscitation skills for the cardiac arrest victim are important, CPR training also teaches potential rescuers how to recognize the signs and symptoms of heart attack and stroke.
More than 50 percent of heart attack patients die before they reach medical care, often from their own delay in seeking medical care. The most common symptom of a heart attack is the denial of symptoms by the patient. Trained employees help increase awareness and recognition of heart attack and stroke, significantly improving survival rates.
CPR Training Quality is Stressed
Cardiopulmonary resuscitation is a technique that allows a rescuer to provide ventilations and circulation to a victim of cardiac arrest. The training has been used to train health care providers, first responders, and the public in how to recognize the signs of a heart attack and provide emergency treatment for cardiac arrest since the 1960s. Yet, despite more than 40 million people having been trained in CPR, the number of cardiac arrest deaths has not been substantially reduced.
Recent studies have demonstrated inadequate compressions and ventilations by health care providers who respond to cardiac arrest in the hospital and by EMS providers. Strong emphasis is now being placed on the quality of CPR training by most agencies who offer training.
CPR training is usually accomplished in a four- to six-hour session that includes management of the heart attack patient, obstructed airway techniques, and CPR for infants, children, and adults. Training for health care providers includes how to operate an AED proficiently. AED training is an option that can easily be incorporated into CPR training programs for lay rescuers.
AED Management, Deployment
Companies initiating an AED program need to do a site survey for AED placement, develop and improve their OSHA-required internal emergency action plan, and select the right AED. AED programs should have strong physician medical oversight, and there should be emphasis placed on training that is site-specific.
It is important to recognize the difference in the various AEDs currently on the market. Listening to sales pitches can be confusing, and this is not the best way to select an AED. (We recently saw an AED sold on eBay for less than half of its original cost. The only problem: The FDA had recalled the device six months before, something the seller failed to mention.)
Technology and ease of operation differ among the brands that are available. Replacement costs for batteries and electrodes should be considered. Some are very cost effective, but some can cost hundreds of dollars a year to properly maintain.
There are no "bad" AEDs. They differ in how they deliver treatment, their capabilities, their features, color, cost, and style. But essentially they all do the same thing: assess a cardiac rhythm and deliver a defibrillation shock. I have often said, "If I go down and you have an AED, put it on me, irrespective of the brand."
Since the first AED was released in 1989, many new products have come to the market. Some are made by companies with a long history of manufacturing medical equipment; others are start-up companies, some of which have experienced serious financial difficulties. One small, financially troubled company recently closed its doors and no longer sells supplies or provides technical assistance for its devices.
This article appears in the June 2005 issue of Occupational Health & Safety.
This article originally appeared in the June 2005 issue of Occupational Health & Safety.