Rethinking SCA at Work
Optimizing one person does not guarantee that an organizational problem will be solved.
HOW a person thinks about a problem influences how he or she plans and responds. In most science--physical, biological, and social--analytic thinking is common. As established in analytic geometry, one axiom of this type of thinking is that "the whole is equal to the sum of the parts." Consider three examples.
First, suppose you want to show a CPR/AED video, but there is a problem: When the play button is pressed on the combination DVD player/monitor, the images on the screen move very slowly and are blurry. Because analytic thinking presumes the "poor play quality" problem is the sum of the parts, one of which would be assumed to be broken, you would assess the performance of each part. You could test the DVD disk by trying to play it in another machine. If it played well, you could focus on the player/monitor by trying to play a different DVD in it, or you could adjust the device settings using the remote control. If these or similar efforts did not reveal the source of the problem, you might contact an expert, who would likely search for the
You could ensure the availability of health care practitioners qualified to provide Advanced Life Support (ALS). Of course, this is the Chain of Survival. Described as an ideal system of emergency cardiac care, it is promoted that if each element is improved or optimized, the probability of overall survival following SCA increases.
failure deeper within the hardware or software. Once the problem part(s) were identified, they would be repaired, enhanced, or "optimized," and the problem should be solved, i.e., the DVD video should play as expected.
Second, suppose your company sells CPR/AED educational products, but there is a problem: During the past year, the number of DVDs being sold has been too low. If the sales manager thinks analytically, she would believe DVD sales are caused by (are equal to) the sum of the parts, one or more of which would be assumed to be broken. She might critically examine the production quality and/or the price of the DVDs offered for sale. If she believed competitors were more aggressive in marketing their products, she might recommend that more or better marketing take place. An analytic thinker would assume that if the inadequate causal parts were optimized, the problem should be solved, i.e., sales should improve. This is depicted in Figure 1.
Third, suppose your company wants employees to have a safe and healthy workplace, but there is a problem: Published data show that the probability of survival following sudden cardiac arrest (SCA) is poor. An analytic thinker would believe that overall survival from SCA is caused by (is equal to) the sum of the parts; if these are optimized, survival will improve. You could reinforce the importance of and ability to quickly alert EMS in case of SCA signals. You could conduct many high-quality CPR/AED courses. You could acquire and carefully place in the workplace the best available AEDs.
Chain of Survivalundefined
Survival Rate = Early Access + Early CPR + Early AED + Early ALS |
But the three examples are not the same. The "poor play quality" problem involves a machine, the parts of which are mechanical and mindless. It would be inconceivable to believe a DVD disk or player would "decide" not to operate as designed. The "poor sales" and "poor survival" problems are organizational where the parts include people and groups who are social and mindful. People have individual interests and goals and make purposeful decisions about their own behavior. People may not act as designed or as expected (hired) when personal interests and behaviors conflict with those of other people or groups. Replacing or optimizing one person does not guarantee that an organizational problem will be solved.
 Systems Thinking
Systems Thinking
Rather than reducing a problem into small pieces, a systems thinking approach assumes certain problems must be examined as a whole because source of the problem is not in any one part, but rather is due to the interaction between the parts. Rather than optimizing a part, a systems thinking approach tries to synthesize or improve the relationships among the parts in order to enhance the whole.
Figure 2 reframes the "poor sales" problem using systems thinking. In an organizational systems problem, sales are both a cause and effect of other activities, many of which interact with other forces and activities. Because interrelationships are complex, it is not clear where to make changes in order to improve sales.
 Reframing SCA Survival
Reframing SCA Survival
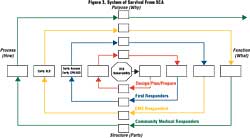
I am arguing that when SCA occurs in the workplace, the varied organizational structures, governance, history, culture, values, policies, and interests of the participants create a complexity for which analytic thinking is inappropriate and misleading. Rather than optimizing each part in the Chain of Survival, the links (parts) should be understood in terms of how they interact with other parts in the overall system. Rather than devoting so much effort arranging for the best CPR training or the most advanced AED--both of which are certainly important--organizations should better understand and manage how these components interact with other parts and how these relationships affect the entire system. Figure 3 presents a reframed System of SCA Survival involving a series of spirals within which the Chain of Survival is located.
When members of an organization recognize there are manageable risks or threats from SCA, this awareness of vulnerability generates the motivation to reduce possible losses, to respond in meaningful and appropriate ways, and to try to improve survival. The first cycle of the system of SCA survival involves efforts to design, plan, and prepare for SCA emergencies. The second cycle addresses the relationship between the planning and the participation of workplace first responders. This is followed by the involvement of EMS responders, then the community medical responders. Because each phase of activity involves operations, parts (including people), procedures, and levels of accountability that interrelate in multiple ways, all spirals are framed in terms of their function, structure, process, and, purpose. In order to ensure the system is aligned and is effective, representatives from each level of organizational activity must understand the scope of the complete problem and must participate in the design of the system needed to control it. Table 1 summarizes the nature of the forces within the system.
 Functional Considerations
Functional Considerations
Functional activities concern what tasks or activities exist and what must be accomplished or controlled across all cycles. I have suggested seven functional categories, but there may be others. To be certain that all functional activities are identified and included, all stakeholders should be clear about the risks, interests, and resources that are currently available from all facilities and personnel. All relevant stakeholders should be clear about all functional tasks because making assumptions about the needs and interests of others can lead to inadequacy, confusion, conflict, and error. Twenty years ago, for example, research1,2 reported that EMS and industry had significantly different perceptions of each other that produced errors of ignorance. Realizing that misperceptions and conflict remain common in 2006, the American College of Occupational and Environmental Medicine (ACOEM) urges that occupational SCA planning should be integrated. ACOEM notes:3
" . . . it is important that information about each workplace AED program be communicated to community emergency medical services (EMS) providers and coordinated with EMS response protocols . . . (and) the workplace AED program should be a component of a more general medical emergency response plan, rather than a freestanding program."
Structural Considerations
The structural characteristics specify the parts necessary to carry out the functional tasks. For example, to address the functional activity of identifying risks for all stakeholders, written plans incorporating the interests and needs of the workplace, EMS, and community medical center are required. Structural parts include information such as written policies, regulations, and documentation; devices, equipment, supplies, vehicles, and technology; services, including follow-up maintenance; and people and groups. Structural integration involves determining what parts are required, what the parts share, and what conflicts and absences exist among parts within and between the cycles (subsystems).
Process Considerations
Process concerns how the functional requirements will be carried out using the structural parts. If CPR/AED knowledge/skill is determined to be an important function (for first responders at the scene, EMS responders, and community medical center responders) and if CPR/AED classes are the parts that will produce an acceptable degree of knowledge/skill, then the process requirement would determine how to ensure training alignment for everyone. Analytic thinking results in the search for training that is best only for the workplace, e.g., classes that are the least costly in terms of resources or the easiest to acquire and manage. A systems framework, however, suggests that because SCA survival is co-produced by interrelationships, CPR/AED training that is systemically coordinated would be better. Perhaps the availability or delivery of CPR/AED training classes could be controlled and/or delivered by joint representatives of the workplace, community EMS, and/or local medical center. This would produce an integrated understanding of the goals, expectations, resources, and competencies among all stakeholders.
Because processes among the subsystems should be integrated, common rather than unique equipment and technology would be preferred. A systems approach suggests a redesign of the communication process. A systems design would have "911" connect from the workplace to EMS dispatch, and EMS responders who would be sent to the scene, and a representative of the hospital emergency department (ED). If the communication roles of EMS and ED personnel were coordinated and empowered, as soon as telephone contact was made, members of the workplace first responder team could share with all members of the emergency system what was happening or not happening; the senior or designated system members could provide feedback, support, and advice. Should patient transport to the ED be needed, all stakeholders would again have continuous information and update. Dedicated communication hardware (cell phone) could be built into or accompany every AED device.
Purpose Considerations
The purpose of the system addresses why the functions, structures, and processes are needed and defines accountability. Overall, the purpose of the system is to increase the probability of survival following SCA and to protect the health and safety of the people and the organizational structures engaged in response efforts of which all are a part. Designing a system to increase the probability of survival for a person at the workplace who collapses due to SCA involving ventricular fibrillation (VF) is an important functional requirement. From a structural perspective, acquiring a device that can be accessed quickly, can be used by workplace first responders to accurately identify and convert VF, and can also interface with the equipment and needs of EMS is appropriate. Acquiring, being able to properly operate, and having quality control (service) for an AED that is acceptable to the needs of all stakeholders would create process alignment. From the perspective of purpose, therefore, this equipment component of planning around SCA risk would be fully integrated in order to protect the health and safety of a person following workplace SCA.
Challenge
I realize this may be controversial, but when a person at a workplace collapses due to SCA, I argue that who will live and who will die is not controlled by optimizing the parts of early access, early CPR, early AED, and early ALS. Many more interrelated forces influence survival. Broadly, part of the causes of survival involve the nature and expectations about people and their work within organizations and how those involved in planning and responding think about reality and information. More specifically, survival involves the details of how preparation and response plans are designed, what components are specified, how the activities are carried out, and why those involved agree to participate. These translate into the degree of perceived threat, quality of planning, governance, structure, culture, education, and resources allocated.
I also argue that the Chain of Survival is not an ideal system; it isn't even a system. Use of a linear chain metaphor promotes analytic thinking and planning. The focus for too long has been on improving individual parts, yet survival following SCA is not controlled by what is done independently at the workplace by first responders or by EMS or by those in a medical center. Rather, improvement in survival rates is to be found when the workplace, EMS, and the community medical groups assume the responsibility of integrating and synthesizing their interests within an overall system. More important for patient survival is to bring together the stakeholders, all of whom have purposes and interests, then align and interrelate them within the whole.
References
- Starr, L.M., Bush, D.F., Borak, J. & Waymaster, S. (1986). Emergency teams, industry have different perceptions of each other. Occupational Health & Safety, 55(6), 20-24.
- Starr, L.M., Borak, J., Bush, D. F., & Waymaster, S. (1986). The hazards of ignorance: The EMS/Industry interface. Journal of Emergency Medical Services, 11(9), 6-7.
- Starr, L. M. (2002). Evidence Based Statements: ACOEM Guideline: Automated External Defibrillation (Reaffirmed in its entirety by the ACOEM Board of Directors on May 6, 2006), available at http://www.acoem.org/guidelines.aspx?id=564&terms=DEFIBRILLATION&searchtype=1&fragment=True#.
Table 1. Functional, Structural, Process, and Purpose Categories of the System of SCA Survival
Design, Plan, Prepare --> First Responders --> EMS Responders --> Community Medical Responders |
CATEGORIES |
FUNCTION--WHAT |
STRUCTURE--PARTS |
PROCESS--HOW |
PURPOSE--WHY |
1. Risk, threat and uncertainty identification, analysis, and control |
What specific risks, threats, and uncertainties from all sources exist and should be controlled when workplace first responders respond to early warning signals; when EMS enters the occupational site to provide further or advanced support; when community medical responders interact with EMS to provide definitive care; when the workplace administration interacts with colleagues and family of the SCA patient after transport and when any of these stakeholders interact? |
Has an SCA risk and hazard identification and assessment document been written?
What is the structure and design of the response activities to be carried out by each stakeholder group individually or when they interact?
What are the shared evaluation and follow-up metrics that will identify "success" and "challenges" for future responses? |
How will all the risk and assessment documents be provided to all relevant personnel?
How will it be assured that all stakeholders understand how to control risks?
How will success of controlling risks be measured? |
Why must the risks and uncertainties associated with SCA be identified and controlled?
Why must there be special controls to account for risks to EMS and community responders?
Why must all stakeholders be jointly accountable for managing SCA risks and threats? |
2. Governance |
What is the appropriate structure of power, authority, and autonomy among all stakeholders when acting separately and when they interact before, during and after SCA?
What is the appropriate governance if the designated personnel are not available or unable to assume responsibility?
What is the appropriate governance if the event increases in scope or complexity? |
Who are the designated administrative parties, responders, and others responsible for governance within each stakeholder group?
What is the defined governance (power structure) among stakeholders during an SCA event?
Who will be responsible if the event increases in scope or complexity? |
How is authority established and monitored for an SCA event?
How will conflicts between interests of administrators, first responders, EMS, and community medical personnel be governed?
How will governance be managed if the event increases in scope or complexity? |
Why is a governance structure required to manage the activities before, during and after an SCA emergency?
Why might governance change when other stakeholders interface and transfer the SCA patient to a higher level of care?
Why might conflict between stakeholders be relevant to the SCA victim or the stakeholders themselves?
Why might the SCA event increase in scope or complexity? |
3. Stakeholders |
What are the criteria associated with being selected to design, respond in and follow-up to an SCA event?
What are the criteria for others from the workplace, from other organizations, or from the community, to be stakeholders?
|
Who are the designers, developers, and first responders at the workplace?
Who are the EMS administrators and responders, and Community healthcare administration and responders?
Who are the workplace department leaders and administrators relevant to SCA emergencies?
Who are other stakeholders at the workplace or from the extended families of stakeholders? |
How are stakeholders notified of their rights and obligations for an SCA event?
How are conflicts between the rights and obligations of stakeholders managed?
|
Why must the interests and rights of many stakeholders be considered in the planning for , management of, and follow-up for an SCA emergency? |
4. Policies and procedures
|
What policies and procedures (HR, legal, medical, productivity, ethical, etc.) from the workplace, EMS and community medical facilities must be considered or be incorporated for an SCA event?
What conflicts between stakeholder policies and procedures are relevant to an SCA event? |
What policies and procedures from all relevant sources have been provided?
What conflicts from all stakeholders have been identified?
|
How are all policies and procedures provided to all stakeholders?
What assurance exists that all policies and procedures are understood by all stakeholders?
How are conflicts between categories of policies (workplace, EMS or community medical) or between obligations to meet policies controlled or resolved by the stakeholders? |
Why must policies and procedures be identified before, during and following SCA?
Why must policies and procedures be understood and adhered to before, during and following SCA?
Why must a resolution between policies and procedures be considered before, during and following SCA? |
5. Education and training |
What education and training competencies are necessary or desirable for those who plan, develop, respond to and follow-up an SCA event? |
What educational content, platforms of delivery and measures of competency (credentials or courses) are acceptable for those from the workplace, EMS, and community medical environment who are responsible for planning, developing, responding to, and following up an SCA event?
What continuous education or training should be available for all participants to ensure sustained competency to manage an SCA event? |
How will education and training be assured, or carried out and assessed for competency?
How will the providers (instructors) of education and training be qualified and sustained?
How will new instructional technologies and platforms be evaluated for equivalency in producing competency?
How will competency to manage the post-SCA event (with the patient's family) be assured. |
Why must education and training competencies be assured for the planning, developing, responding and following up of an SCA event?
Why must trainers and educational systems be sustained?
Why must the instructional technologies be examined?
Why must there be an educational consideration for dealing with the SCA patient's family after an event? |
6. Technology and equipment |
What technology and equipment requirements are relevant to planning, developing, responding to and following up an SCA event?
What adjustments between technology or equipment may be anticipated when stakeholders interface?
What quality, support or service is relevant for performance of technology and equipment? |
What devices, equipment, vehicles, or technology will be needed ensure the effective planning, development, response and follow up for all stakeholders in an SCA event?
What interface or adjustments between technology or equipment during the interface of stakeholders has been made?
What support or service for technology and equipment has been established? |
How will the technology and equipment be acquired by each stakeholder group?
How will each stakeholder learn how to use the technology and equipment when working independently and when interacting?
How will the quality and service of technology and equipment be carried out and assured by each stakeholder group? |
Why is technology and equipment needed in planning, developing, responding and following up to an SCA event?
Why must technology or equipment be integrated by stakeholders?
Why are quality and service important? |
7. Communication processes and systems |
What communication requirements are relevant to planning, developing, responding and following up of an SCA event?
What measures of communication effectiveness are relevant?
What back-up or redundant communication processes and systems are appropriate? |
What communication processes (procedures) and systems (equipment or platforms) have been provided to carry out SCA survival planning, responding and follow-up?
What measures of communication effectiveness have been established?
What back-up or redundant communication processes and systems have been established? |
How are the communication processes and systems acquired, implemented, and assessed for accuracy and proper use by all stakeholder groups? |
Why are communication processes and systems needed for design, planning, responding and follow-up to SCA events? |
This article appeared in the February 2007 issue of Occupational Health & Safety.
This article originally appeared in the February 2007 issue of Occupational Health & Safety.