
The Aging Worker in the U.S. Construction Industry
Reducing the physical demands on all workers in construction is essential.
- By Laura Welch
- Mar 01, 2010
Construction workers, like the rest of the U.S. population, are getting older. The average age in construction was 40.4 years in 2008, 4.4 years older than in 1985 (see Figure 1). More than 40 percent of construction workers are "baby boomers," that is, they were born between 1946 and 1964. The proportion of construction workers in this age range varies from 23 percent among roofers to 54 percent among construction managers. And construction workers overall stop working at an earlier age than other workers. These demographics predict an exodus of experienced workers from the industry in the next decade. CPWR -- The Center for Construction Research and Training is evaluating ways to increase work participation as construction workers age.
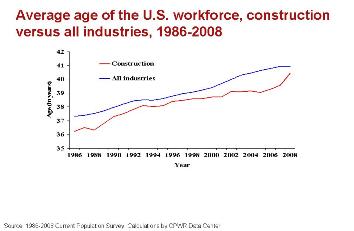 Figure 1 at left depicts the age of workers in the United States over time. Because of the physical demands of the work, construction workers who are employed have to be healthier than the general population, but the same physical demands cause workers with injuries or illness to leave the industry. We know that 10 percent of construction workers do not return to work after an injury, and that construction workers with a musculoskeletal disorder (MSD), lung disease, or injury are more likely to retire on disability than workers with the same conditions in less physically demanding work.
Figure 1 at left depicts the age of workers in the United States over time. Because of the physical demands of the work, construction workers who are employed have to be healthier than the general population, but the same physical demands cause workers with injuries or illness to leave the industry. We know that 10 percent of construction workers do not return to work after an injury, and that construction workers with a musculoskeletal disorder (MSD), lung disease, or injury are more likely to retire on disability than workers with the same conditions in less physically demanding work.
And even without an injury or an MSD, construction workers have a high risk for serious diseases down the road. Construction workers in the United States have the highest rate of smoking among all occupations, at 37.7 percent, compared to a national average of 22 percent, carrying a risk for lung cancer and chronic lung disease. Forty-three percent of U.S. construction workers are overweight, compared to 35 percent of all workers, with a risk for diabetes and heart disease. Because construction work includes a lot of material handling, awkward posture, and other physical demands, many construction workers also develop work-related MSDs, such as chronic low back pain or shoulder problems. Research shows that a worker will retire early if his work is physically demanding or his workplace has limited opportunity for job accommodation; these factors are prevalent in construction. If one looks at the increasing age of workers in this industry, the likelihood of a construction worker developing an MSD or other chronic disease, combined with the industry characteristics mentioned, one can anticipate a shortage of experienced workers in the next decade.
Addressing Major Risk Factors
Work ability is a measure of the balance between work and personal capacity; older age is linked to a reduction in both quality of life and work ability. The Work Ability Index (WAI) was developed in the early 1980s to identify factors that would sustain work as workers age. The questionnaire is now available in 26 languages and is commonly used in research worldwide. Physical work load is an important determinant of work ability among construction workers, and in turn work ability is highly predictive of disability among construction workers. A construction worker between the ages of 45 and 54 with a low Work Ability Index and severe low back pain has a 40-fold increased probability of disability retirement compared to a construction worker without those risk factors. New research shows that reducing obesity, smoking, and manual materials handling, plus improving the worker's control over his own work tasks, can keep construction workers successfully employed.
A study among construction roofers in the United States demonstrated that workers over 55 had lower physical functioning and were more likely to have both a chronic medical condition and an MSD. Consistent with the prior research noted above, older age, reduced physical function, and lack of job accommodation among these roofers were each predictive of early retirement. This study also found that construction roofers who had received job accommodation for an MSD or a medical condition were four times less likely to retire compared to workers with similar medical status but without accommodation. Some form of job accommodation was offered to more than 30 percent of the workers in the study, and many of the accommodations were relatively simple, such as allowing more time to accomplish a task or changing the work schedule; few employers provided new tools or equipment.
These findings are not all that surprising, since we know from research in other industries that job accommodation reduces disability and that vocationally oriented multi-disciplinary rehabilitation programs reduce sickness absence and delay retirement. However construction job sites are by definition temporary and mobile. The absence of steady employment relationships may discourage job accommodation; the employer may be more likely to hire a new worker than accommodate an injured one. An intervention program for construction workers in the Netherlands demonstrated that such programs are both feasible and effective in the construction industry. More information on the effectiveness and cost-benefit of job accommodation in US construction is needed.
Other Interventions
So how can we keep construction workers active and productive at work? A program developed in Finland to promote work ability and prevent premature retirement among all workers identified 4 important areas: improvement in work demands, improvement in work organization, promotion of the worker’s health and function, and promotion of the worker's professional competence. Relevant research initiatives at CPWR are focused on (1) improving safety culture and work organization, (2) implementing design for safety to reduce injury and MSDs, (3) identifying solutions to reduce the physical demands of work, and (4) reducing the burden of chronic disease among construction workers. Success in each of these areas requires both understanding how the construction industry is different from other industries, and taking advantage of its special characteristics. The work is physically demanding and every changing. The industry values field innovation, and respects the skills and autonomy of the craft worker. Given these factors, participation of workers, trade unions, and contractors is essential in the development of solutions to improve work ability.
Reducing the physical demands on all workers in construction is essential. Success will require changing the culture of construction, developing new task-specific ergonomic innovations and promoting participatory ergonomics programs for this industry. The construction work environment changes as a project moves through various stages of construction, workers change to new work locations frequently as projects are of relatively short duration, and the majority of construction work occurs at the ground and ceiling levels, placing workers in awkward postures for the majority of their work. By understanding these challenges, researchers have developed effective interventions that can reduce physical demands in construction. These interventions include reducing back stress in masons through adjusting work height, eliminating shoulder strain during overhead drilling tasks with a drill support, and a variety of approaches to reduce manual materials handling.
At the same time, CPWR and partners have identified important factors that facilitate or impede interventions for this industry. Interventions that are more likely to succeed have a relative advantage, are compatible with prevailing norms or practices, can be tried before being implemented, and have a readily observable impact. CPWR is planning a rigorous analysis of a participatory ergonomics program for construction workers to gather data on these and other factors that enhance or impede adoption of solutions for the high physical stress in construction.
Improved safety culture is associated with reduced injury, better compliance with PPE, and other factors. One CPWR project is working with pipefitters and plumbers and their employers from three geographical regions. Activities include: (1) surveying worker and contractor representatives to identify barriers to safe working behavior considered to be most prevalent and severe; (2) implementing training programs for worker and contractor representatives that address ways to alleviate these barriers; and (3) assessing the effectiveness of these training programs for reducing barriers, increasing safety behaviors, and decreasing injuries (4) developing the most attractive and effective dissemination channels of safety research findings based on focus groups of worker, contractor, and other safety representatives: (5) tailoring safety campaigns to worker and contractor representatives; and (6) evaluating the effectiveness of the safety communication campaigns for increasing knowledge and awareness about construction safety barriers. Although not yet proven, it is likely that companies with a good safety culture would be more successful in implementation of a participatory ergonomics program, as well.
Health promotion programs are needed to reduce obesity and smoking among construction workers, and programs that integrate health promotion with information on occupational hazards in construction have been shown to be more effective than health promotion alone. Occupational physicians have worked successfully with labor unions on effective health promotion/health protection programs and helped change the social context for smoking and other risk factors for chronic disease. CPWR is partnering with health and welfare funds in the construction industry to implement evidence-based disease management programs, with an initial focus on diabetes and cardiovascular disease; the evaluation will include measurement of both the costs and the quality of medical care provided.
Now that factors affecting work ability among construction workers have been identified and effective tools and approaches to these factors described, the construction industry and the occupational health community need to increase the range and scope of programs to reduce physical demands, reduce obesity and smoking, and improve work ability. New technologies, educational materials, Web sites, and training workshops alone are not sufficient to improve the work environment and work ability. Successful implementation of rehabilitation programs, ergonomics and health promotion require integration and implementation of these programs within the community of construction. Let's get to work.
CPWR is a 501(c)(3) nonprofit research and training institution created by the Building and Construction Trades Department, AFL-CIO, and serves as the research arm of the BCTD. For more information, visit www.cpwr.com.